This retrospective study looked at trauma patients over age 65 and divided them into age ranges 65-80 (geriatric) and 80 plus (super-geriatric). They then looked at mechanusm of injury, mortality, interventions,etc. What they found was ages 65-80 were more likely to be injured in motor vehicle crashes vs. falls for those over 80. Those over 80 received less interventions including hemmorhage control surgery and had much higher levels of withdrawal of care.
This study highlights that the geriatric population is not as a monolithic group over age 65, but more nuanced by various age ranges over 65. Research going forward should be adjusted to these nuanced age ranges. Out treatment approaches should be adjusted in geriatric vs. super-geriatric patients as well.
A recently published study of ED APPs, residents, attendings, and nurses attempted to assess clinician's perspectives on how ED boarding impacts ED staff and patients. Authors performed a survey followed by focus group sessions to obtain qualitative insignts from participants.
All respondents associated boarding with feelings of burnout and self-reported poor satisfaction with communication and the process of boarding care.
Several key themes emerged which are outlined below:
This publication highlights the negative workforce and patient safety effects of ED boarding. It amplifies the voices of our colleagues who work towards change to improve both the health of our wrokforce as well as that of our patients and the communities that we serve.
Acute bronchiolitis (AB) is a common cause of respiratory tract infections in infants. A recent study looked at the application of Point-of-Care Lung Ultrasound (LUS) in infants <12 months who presented with symptoms of AB.
They scored infant lungs using a cumulative 12-zone system. With the below scale:
0 - A lines with <3 B lines per lung segment.
1 - ≥3 B lines per lung segment, but not consolidated.
2 - consolidated B lines, but no subpleural consolidation.
3 - subpleural consolidation with any findings scoring 1 or 2.
They found that infants with higher LUS scores had increased rates of hospitalization and length of stay.
Here are some tips for ultrasounding a pediatric patient:
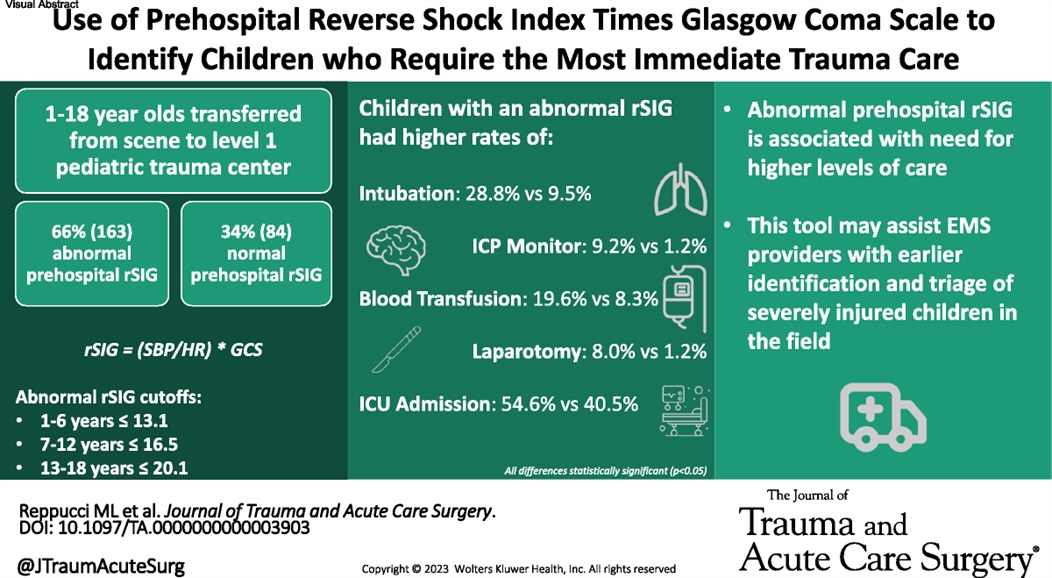
This small study suggests using reverse shock index times the Glasgow Comma Scake score may give a prognostication on pediatric trauma severity and resource utilization.
This disturbing study out of the UK details the prevelance of sexual harassment, sexual assault and rape within the hospital environment.
Overall it's clear that women surgeons in this study were the victims and witnesses of sexual violcence at a substantially higher rate than men. 89% on women report being witnesses of sexual harassment and 63% being the victim of it; 30% of women report being the victim of sexual assault, and 35% report being witness to it; and most concerning 0.8% of women report being raped by a colleague, with 1.9% being witness to it.
The study also asked respondents about their faith in higher organizations' (the Royal Colleges and the General Medical Council) ability to respond to these issues. For women, the percentage of people who felt that there was an adequate response was only between 15-30 percent.
There is a huge and persistent gap between men and women both witnessing and experiencing sexual harassment and assault at work. Everyone has a responsibility to immediately interrupt any form of sexual harassment or assault, no matter how inocuous it may seem to the perpertrator, in order to provide an environment we can all thrive in.
This pediatric ICU study measured ICP during and after ketamine infusion. There was no increase in ICP associated with the ketamine infusion. This small study adds to the data that ketamine is safe in pediatric brain injured patients.
https://prod-images-static.radiopaedia.org/images/626179/d58f35a8aa4a0a6750a6adce4087a4_gallery.jpg
"I was kicked in the inside of my knee while it was straight (extended). Look at the x-ray and tell me if its bad"
For the folks who have been in practice for a while, you may be aware of the roller-coaster evidence base looking at steroids for pneumonia. Once thought to be beneficial and clearly indicated, of late steroids for pneumonia have fallen out of favor. Hamad et al have published an excellent (and brief) review in Clinical Infectious Diseases which suggests the pendulum might be swinging back in favor of giving steroids to patients with pneumonia. It's a ~5 minute read, so I recommend glancing through it yourself, but below are my two cents (solely my opinion) on where we are with steroids for pneumonia.
Take Home Points (OPINION ALERT):
1) When you have a condition present that you consider an indication for steroids (e.g. severe COVID-19 for sure; septic shock, s. pneumo infection, and ARDS depending on how you feel about the existing literature) --> strongly consider giving steroids unless there's a contraindication
2) When you have an undifferentiated patient who MAY have one of these conditions (e.g. pneumonia with COVID pending, patient potentially in ARDS or high risk of going into ARDS, etc) who is very sick --> it is reasonable to give steroids (if no contraindication) or not give steroids. My tendency is to lean towards giving steroids in these cases, but do be aware that society guidelines recommend against steroids here (although debatable if they just haven't caught up to more recent literature)
3) When you have an undifferentiated patient who may have one of these conditions, but is NOT very sick --> I do not think there is significant enough evidence to support empiric steroids
4) Factors that might push you one way or another:
Think before placing a nasogastric tube!
Multiple articles which discussed complications of NGT placement were included in this integrative review, with the majority (n=67) publishing results in English. The authors categorized adverse events into two broad categories:
1) Mechanical adverse events - including respiratory, esophageal, and pharyngeal complications, obstructed tube, intestinal and intracranial (!) perforation, and tube withdrawal
-The largest cohort (n=44) was respiratory, with displacement or placement of tube to the respiratory tract
2) Others - pressure injury and misconnection
-One study showed pressure related injury in 25%, and 5 articles discussed complications of misconnection (including extravasation of gastric fluids and inadvertent connection to central venous catheters)
16 of the 69 studies reported death as a consequence of improper placement.
One big takeaway: there is no universally accepted standard for verificaiton of tube placement. Xray is considered to be *most* accurate. Tubes should also be checked periodically and depth should be marked. Evidence-based guidelines need to be developed to improve patient safety, outcomes, and quality of care.
This systematic review and analysis found in 1822 trauma patients treated with ECMO:
-Overall 66% survival to discharge
-VV ECMO was significantly superior to VA ECMO
-Mean age was 35 years. Typical of ECMO use in trauma is younger healthier patients are chosen to receive ECMO
“ECMO is not a routine life-saving intervention following trauma, but rather a salvage therapy that effectively replaces conventional treatment for young, healthy patients when conventional methods fail. Its complexity requires a multidisciplinary healthcare team and sufficient resources for optimal implementation.”
Spanish investigators conducted a 6-month, prospective, observational study to determine the impact of emergency department pharmacists on medication errors. They specifically focused on so called "High Alert" medications and on errors that, if undetected prior to administration, were likely to have serious deleterious consequences.
Over the course of the study, the pharmacists reviewed the medication records and histories of nearly 3000 patients. The pharmacists intervened in the care of 557 patients. Errors were most often detected during the process of medication reconcilliation. Over half of the potential errors were considered "severe" and the majority of pharmacist interventions were deemed important to the patient's care. Many of the medication errors detected involved "High Alert" medications.
The Bottom Line: Pharmacists are integral members of a high-functioning emergency department team. Their specialized knowledge contributes to a safe and effective care environment.
BACKGROUND: Prehospital (EMS) clinicians are positioned on the front lines of health care. With respect to stroke identification and treatment, early recognition is essential to positive outcomes. Considerable variability exists within EMS documentation. Despite considerable variability in documentation, the establishment and tracking of core stroke metrics serves as a benchmark to gauge performance and outline strategies for improvement.
METHODS: Authors conducted a retrospective, observational analysis of EMS encounters (2018-2019) which ultimately received a diagnosis of an "acute cerebrovascular event." Hospital based diagnoses included: hemorrhagic stroke, ischemic stroke, or transient ischemic attack. The data set was comprised of a statewide EMS documentation and a state wide acute stroke registry. Authors examined compliance with six core performance metrics which included measurement of blood glucose, documentation of last known well time, and on-scene time < 15 mins for patients with suspected stroke. During the 18 month study, almost 6000 encounters met criteria for inclusion.
RESULTS: EMS documentation remains a significant source of variability. EMS crews were largely compliant with blood glucose measurement. However, last known well time had the lowest (24%) documentation rate. Patients diagnosed with subarachnoid hemorrhage had the lowest rate of compliance with metrics.
BOTTOM LINE: Accurate prehospital stroke diagnosis remains a challenge. Consistent data collection and benchmarking remains an important first step in the evaluation of performance. Higher NIHSS scores and ischemic strokes are linked to higher rates of metric compliance.
Term? Tone? Tantrum?
Immediately after delivery, your initial neonatal assessment should evaluate for:
- Appearance of full or late pre-term gestation (>34 weeks)
- Appropriate tone (flexed extremities, not floppy)
- Good cry and respiratory effort
Newborns meeting this criteria should not require resuscitation. They can be placed skin to skin on mother and allowed to breastfeed. Delayed cord clamping for 60 seconds is recommended, as data shows improved neurodevelopmental outcomes and iron stores in first year of life.
Neonates not meeting these criteria should be brought to the warmer for resuscitation, with the focus being on:
- Warm - via radiant warmer. Maintain temps 36.5 C – 37.5 C
- Dry - Neonates have thin skin and lose heat readily from evaporative loses
- Stim - tactile stimulation on the head, midline of the back and extremities to provoke a cry and encourage respiratory effort
Avoid routinely bulb-suctioning unless there is significant obstructing mucous, as this can increase vagal tone and result in bradycardia. If bulb suctioning is used, first suction the mouth before the nose.
Majority of resuscitations do not require additional support, however if heart rate is <100 or there is poor respiratory effort, the physician should initiate PPV.
PPV settings: PIP 20 PEEP 5 FiO2 21% Rate of 60 breaths per minute
Improvement in the neonate’s HR is the primary indicator of effective PPV!
If HR poorly responding (remains <100), ensure appropriate mask size, reposition, suction, and increase PIP (max 35) and FiO2.
If HR drops below 60, intubate with uncuffed ETT
- Prioritize adequate ventilation as this is the highest priority in neonatal resuscitation
- Initiate compressions at rate of 120/min.
- Epi dosing is 0.01-0.03 mg/kg q3-5 min
- ETT size estimation by gestational age:
25 weeks = 2.5, 30 weeks = 3.0, 35 weeks = 3.5, 40 weeks = 4.0
IV Fluid Resuscitation
This large UK and US study looked at the addition of high dose cryoprecipitate to mass transfusion protocols and found: “Among patients with trauma and bleeding who required activation of a major hemorrhage protocol, the addition of early and empirical high-dose cryoprecipitate to standard care did not improve all cause 28-day mortality.”
The objective of a recent study was to analyze the injury and illness characteristics in Iron Man distance triathletes. This information is important for emergency providers who may be asked to directly assist or help coordinate race day medical care.
Intro: The Iron Man distance triathlon is one of the most challenging ultra endurance competitions in the world. 80,000 Iron Man triathletes compete internationally each year to qualify for the Ironman world championship. The race totals 140.6 miles across three legs, beginning with a 2.4 mile swim, followed by a 112 mile cycle, and is completed with a 26.2 mile run.
Retrospective cross-sectional study of medical records from Iron Man distance championship races across a 30-year period (1989-2019). The study population (10,533) consisted of all triathletes treated at mobile medical units along the race route or who presented to the medical tent for evaluation during and immediately after the event.
Mean population age of 37 with a range of 18 to 87 years.
Results: Female athletes were found to present to the medical tent more than males (P < 0.001).
The total incidence of medical encounters by age was found to be higher in both younger athletes (18 to 34 years old) and older athletes (greater than 70 years old) versus middle-aged athletes (35-69 years old) (P < 0.001).
Professional athletes have similar overall medical encounters compared with other athletes.
The busiest hours of the medical tent were between approximately 9 and 14 hours after start time (afternoon and early evening) in which approximately 73% of athletes presented for evaluation and treatment.
Once inside the medical tent 71% of athletes were discharged within an hour and 87% were discharged within 1.5 hours. Athletes were dispatched to the hospital from the medical tent area at a rate of 17.1/1000 athletes (most athletes presenting to the medical tent finished the race and few required hospital transfer).
The most common medical complaints were dehydration and nausea followed by dizziness, exhaustion, muscle cramps, and vomiting.
Blood work was collected for 30% of athletes who entered the medical tent. Of these athletes, hyponatremia was the most prevalent diagnosis and most of whom were symptomatic with symptoms such as confusion, stupor, gait disturbance, muscle weakness, headache, dizziness, fatigue, nausea and vomiting.
Beyond basic medical care, intravenous fluids were the most common medical treatment.
Conclusion: Medical events were more frequent among female athletes as well as both younger and older age categories. Gastrointestinal and exertional related symptoms were the most common complaints in the medical tent. Besides basic medical care, IV infusions were the most common treatment. Most athletes presenting to the medical tent finished the race and only a small percentage were transferred to the hospital.
This excellent review article discussing damage control resuscitation in traumatically injured children highlights several points including:
-”Damage-control resuscitation (DCR) consists of rapid control of bleeding, avoidance of hemodilution, acidosis, and hypothermia; early empiric balanced transfusions with red blood cells, plasma and platelets, or whole blood when available, and the use of intravenous or mechanical hemostatic adjuncts when indicated.”
-”he 30-day mortality in children with traumatic hemorrhagic shock is estimated to be 36% to 50% compared with the 25% reported mortality in similar adults. The early stages of hemorrhagic shock after injury in children can be more challenging to recognize because of their remarkable compensatory mechanisms. In children unlike adults, blood pressure alone is an insensitive indicator of hemorrhagic shock as hypotension is a late sign often not occurring until blood volume is reduced by >40%.”
-”Based on the current literature, the challenges health care providers must focus on are the early recognition of shock in the pediatric patient, moving the hemostatic resuscitation forward to the prehospital phase when feasible, improvement in times to first blood product, balanced resuscitation and efficiency of massive transfusion protocols (MTPs).”

{kind=link}